Anthrax is a peracute to acute, febrile, infectious disease caused by the bacterium Bacillus anthracis. While it is famously known as a potential agent of bioterrorism, for the veterinary practitioner, it remains a critical soil-borne zoonosis that demands immediate recognition and strict regulatory adherence. Understanding the unique survival mechanisms of the pathogen and its clinical manifestations across various species is essential for both animal welfare and public health.
The causative agent, Bacillus anthracis, is a Gram-positive, rod-shaped, facultative anaerobic bacterium. Its pathogenicity is defined by two primary virulence factors encoded on plasmids (pX01 and pX02): a poly-D-glutamic acid capsule that inhibits phagocytosis and a tripartite exotoxin consisting of Protective Antigen (PA), Edema Factor (EF), and Lethal Factor (LF).
The true challenge of anthrax lies in its lifecycle. When exposed to oxygen—typically when a carcass is opened or when the bacteria are shed in terminal hemorrhages—the vegetative cells undergo sporulation. These spores are incredibly resilient, surviving for decades in "alkaline spore beds" (soil with high calcium and organic matter). They are resistant to desiccation, heat, and many standard disinfectants, making environmental management a long-term struggle.
In livestock, transmission occurs primarily through the ingestion of contaminated soil, forage, or water. Outbreaks often follow periods of climatic stress, such as heavy rains or droughts that expose deeper soil layers or concentrate spores in receding water holes. Inhalation is a rarer route in veterinary medicine but can occur in dusty environments.
Once spores enter the host, they are germinated by macrophages and transported to regional lymph nodes. The vegetative bacteria then enter the bloodstream, leading to massive septicemia. The toxins produced cause:
Anthrax presents differently depending on the host's susceptibility:

The most critical takeaway for any veterinarian is the prohibition of field necropsies on suspected anthrax cases. Opening the carcass provides the oxygen necessary for the vegetative cells to sporulate, contaminating the environment for generations.
Diagnostic Indicators:
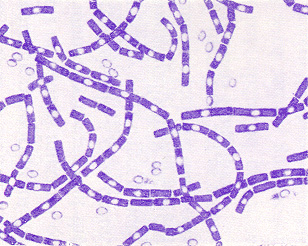
For confirmation, a peripheral blood smear (or a swab of exudate) should be collected aseptically. Under Polychrome Methylene Blue (M’Fadyean) stain, the bacteria appear as blue rods surrounded by a pink-to-purple capsule.
Anthrax is a notable disease; authorities must be informed immediately upon suspicion.
Treatment: In early stages or exposed herd-mates, high doses of Penicillin or Oxytetracycline are effective. However, treatment is often futile once clinical signs are advanced.
Animals under treatment should be isolated.
Vaccination: The Sterne-type live spore vaccine is the global standard for livestock in endemic areas. It should be administered annually, at least 2–4 weeks before the expected "anthrax season."
Postmortem examination is NOT recommended in suspected anthrax cases.
Reason:
Opening the carcass exposes vegetative bacteria to oxygen → spore formation → environmental contamination.
Typical findings (if observed externally):
Carcass Disposal: Carcasses should be burned completely or buried deep (at least 6 feet) with a layer of quicklime (calcium oxide) to prevent scavenger access and spore movement.
As a zoonotic disease, humans can contract anthrax through contact with infected tissues (Cutaneous), ingestion (Gastrointestinal), or inhalation. Practitioners must use rigorous Personal Protective Equipment (PPE) when handling suspect cases to avoid "Hide-porter's disease" or accidental inoculation.
